


2 potential treatments for post-vax damage
Agonistic autoantibodies, DRACO

In the following article I want to present you the correlation between autoantibodies and certain side-effects such as cardiac issues which a lot of us are experiencing now.
Even prior to these novel injections autoantibodies are accounted for a variety of specific diseases like dementia, dilated cardiomyopathy and thromboangiitis obliterans.
I want to emphasize that autoantibodies are only a part of the problem beside the findings of graphene oxide capped with PEG, quantum dots and heavy metals in the shots.
However, the removal/neutralization of these autoantibodies has shown significant improvement of neurological as well as heart related issues for some patients.
Autoimmune diseases such as dementia and dilated cardiomyopathy are on the rise.
What are the potential causes and how to mitigate them?
Autoantibodies
Autoantibodies are directed against specific receptors on the cell surface, namely G protein-coupled receptors (GPCR).
The GPCR superfamily comprises several hundred receptors. GPCRs are found in all cell types of human and animal tissues. They mediate the action of a variety of signaling substances such as hormones, neurotransmitters and even photons. Of many GPCRs, the natural ligands are not yet known. GPCRs are involved in regulation of almost all bodily functions. They control many physiological processes and often play a central role in pathological conditions role. They are therefore the most important target structure for pharmacological therapeutic approaches. All GPCRs consist of an unbranched chain of amino acids, which penetrates the surface membrane of the cell seven times 1
The physiological activation of the GPCR occurs through binding of the respective agonist to the extracellular binding site and the subsequent intracellular linkage of two receptor molecules (dimerization). 1
Depending on the type of G proteins recruited by the receptor G proteins, cellular signaling pathways are activated or inhibited.
Adrenergic receptors (adrenoceptors) such as α-adrenergic and β-adrenergic GPCRs are a type of GPCR that regulate the activity of the sympathetic nervous system.
There are α1, α2 and β1, β2, β3 receptors.
The adrenal medulla produces neurotransmitters/hormones such as adrenaline and noradrenaline which function as natural ligands towards these adrenergic recetpors.
Among other physiological processes, adrenoceptors regulate cardiac and vascular musculature and are used as target structures in diseases of the myocardium and vascular system such as such as heart failure and hypertension, are of immense therapeutic therapeutic importance. 1
Affected tissues and organs and the severity of the symptoms result in differing autoimmune diseases. Certain autoimmune diseases are characterized by the appearance of antibodies (agonistic autoantibodies) that bind at GPCR (g-protein coupled receptors) and activate them.
Example of autoimmune diseases the paper [1] addresses: dilated cardiomyopathy as well as common diseases such as hypertension, type 2 diabetes and dementia. Hence, the focus is on the α1-adrenergic receptor (α1-AR).
This GPCR is involved in regulation of contractile myocardial function and glucose metabolism and is central to vascular muscle function. Antibody diagnostics of patient sera showed a striking occurrence of agonistic autoantibodies against the α1-AR in diseases with prominent vascular prominent vascular involvement. This suggest that autoantibody-induced unphysiological activity of the unphysiological activity of the α1-AR may be a pathomechanism for vascular damage, which is an essential and important factor in severe diseases such as dementia and type 2 diabetes, if not a causal role.
Agonistic autoantibodies trigger receptor-specific reactions in the cell through activation of the GPCR. These reactions may be, but necessarily identical to those activated by physiological agonists.
Pathological conditions can be calcium overload of the cells, the remodeling of cell structures (remodeling) up to cell death.
Considering the importance of the α1-AR for the function of the smooth muscle function, a decisive role of agonistic autoantibodies attacking this receptor in the development of vascular damage must be assumed. The vascular damaging potential of antibodies directed against the α1-AR was shown for the first time in rats immunized with the corresponding receptor peptides (14). The immunized animals developed antibodies against the α1-AR and showed pathological changes in peripheral vessels such as aorta and mesenteric arteries (Fig. 1).
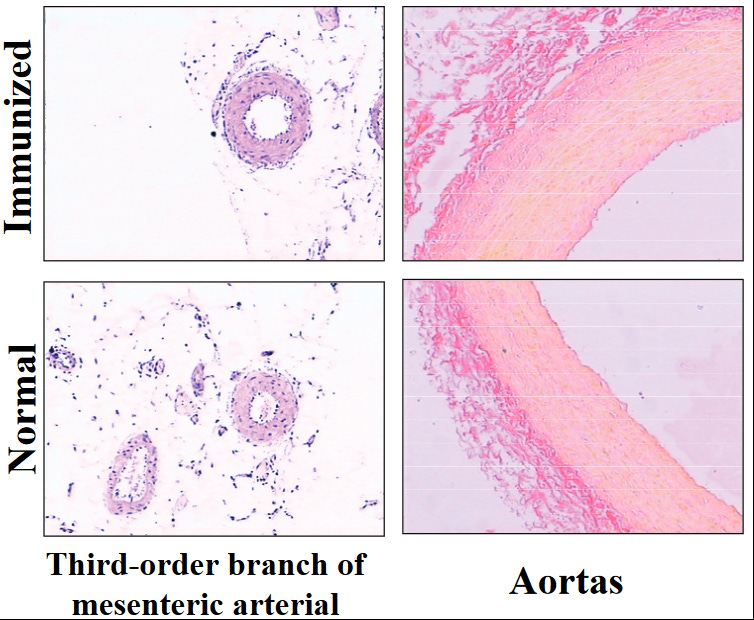
Fig. 1. pathological changes in the mesenteric artery and aorta of immunized rats in which antibodies against the α1-adrenoceptor were were induced. The thickened vessel walls are the result of increased cell hyperplasia.
I sent a blood sample to a lab that is specialized in these autoantibodies back in 2022.
These are the results:
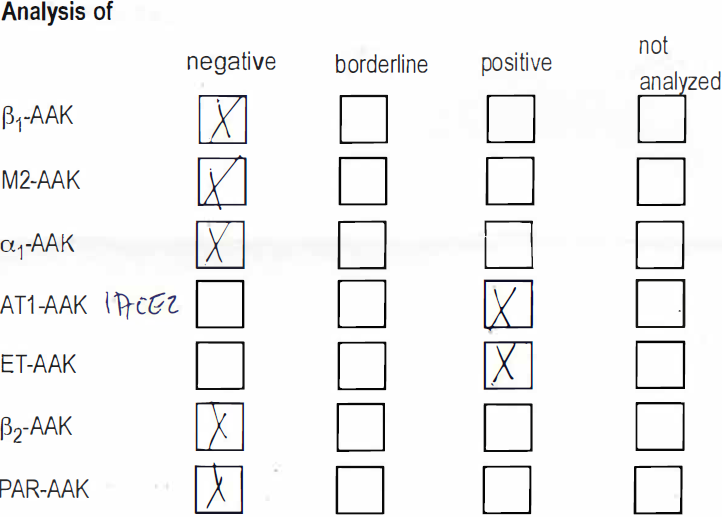
I’m negative for both α1 and β1 autoantibodies, but I’m still suffering from heart problems and daily chest pain. Prior to the test I had a 30 min phone conversation with Ms. Bimmler, the head of the lab that offers these tests. She was afraid to mention the shots as the root cause, but stated it’s an indirect mechanism where the body generated autoantibodies to battle the spike protein and other foreign invaders. According to her data only 15 out 4000 people have autoantibodies. Most importantly they are not a component of the body. But ever since the shots were rolled out she saw an unusual spike of autoantibodies in people from all age ranges. She was friendly enough to recommend me Dr. Erich Freisleben, who later on helped me tremendously with his detailed blood test and referral to the DHZ (German Heart Center). He’s also one of the few doctors in Berlin that know about agonistic autoantibodies and their impact on the human body.
Vascular damage in the brain that leads to dementia is caused by α1-AR and can be shown via TOF MRA scans of rat brains which were treated by α1-AR.
After a period of 8 months, magnetic resonance angiography (MRA) showed a significant reduction in the perfusion of macrovessels in the antibody-exposed animals (Fig. 2).
Antibodies to the α1-AR both damage the macrovascular and microvascular vasculature.

Figure 2. TOF-MRA of rat brain.
Three-dimensional coronal views of the frontal brain segment. The rat shown is as in Figure 3 which was immunized with the α1-AR peptide. Angiographs of the same animal were taken at the beginning of the treatment (A, C) and eight months later (B, C). C, D show the same brain segment as in A, C but vertically rotated by 45°. The defects in blood flow in the right part of the brain as displayed in Figure 3 are obvious (B, D) compared to the situation eight months before (A, C).
Further microscopic analysis of tissue preparations from these animals showed, that the vascular damage caused by antibodies was not limited to the brain region, but also occurred but also occurred in the kidney.2
The paper [1] is discussing 2 therapeutic options:
1. Functional elimination of the agonistic autoantibody
2. Removal of the agonistic autoantibody from the bloodstream
1. Functional elimination of the agonistic autoantibody
The goal of such an approach is to prevent the interaction of the antibody with the affected GPCR. This can be done pharmacologically by receptor antagonists, which are known to weaken the binding of the autoantibody through conformational changes of the receptor molecule antibody and thus detach it from the receptor. To most of the disease-relevant GPCRs receptor antagonists already exist and are used clinically. This option is cost-effective and can be applied to a applicable for a large number of patients. The disadvantage is that pharmacological substances can be associated with considerable side effects and, of course, also affect the also influence the physiological receptor function.
Another principle uses the specificity of the antibody for its antigen.The binding epitopes at the receptor, e.g. the extracellular loop involved,have been elucidated for a number of disease-associated autoantibodies. Low-molecular-weight compounds can be developed here, peptides and their modifications are suggested, which can be specifically bind to the circulating autoantibodies and functionally neutralize them.
A promising candidate for this form of treatment seems to be the aptamer BC007 aka ARC183 by Berlin Cures.
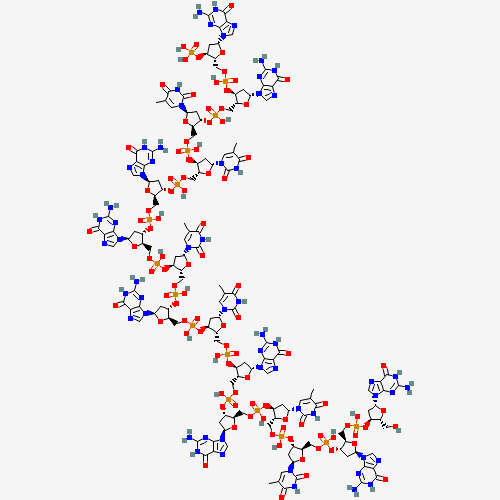
ARC183 is a DNA aptamer, which is a single-stranded DNA molecule consisting of 15 deoxynucleotides that forms well-defined three-dimensional configuration, allowing it to bind to thrombin with high affinity and specificity. The key advantage of ARC183 compared to other thrombin inhibitors is its rapid onset of action and short half-life, giving it the potential to be an ideal agent for medical procedures that require rapid resolution of anticoagulation or that require reversal of anticoagulation shortly after the procedure is completed.3
The aptamer consists of 9 deoxyguanosine and 6 thymidine units.
2D structure of ARC 183:
They are currently in the middle of phase II clinical trial.
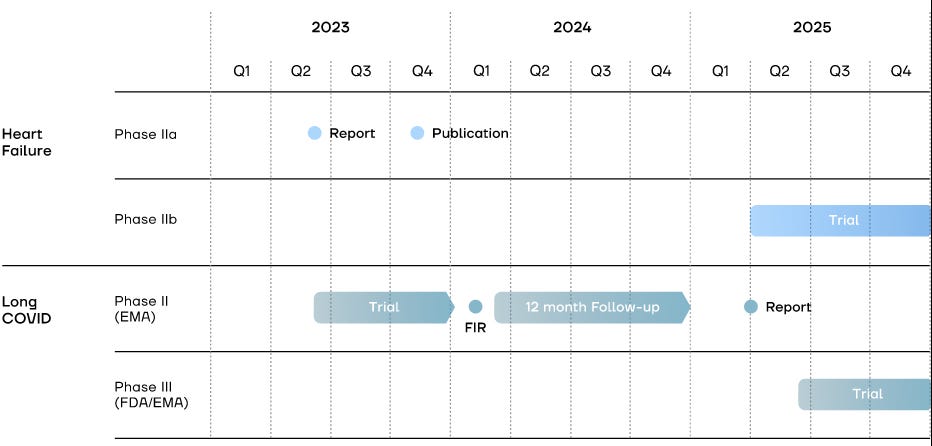
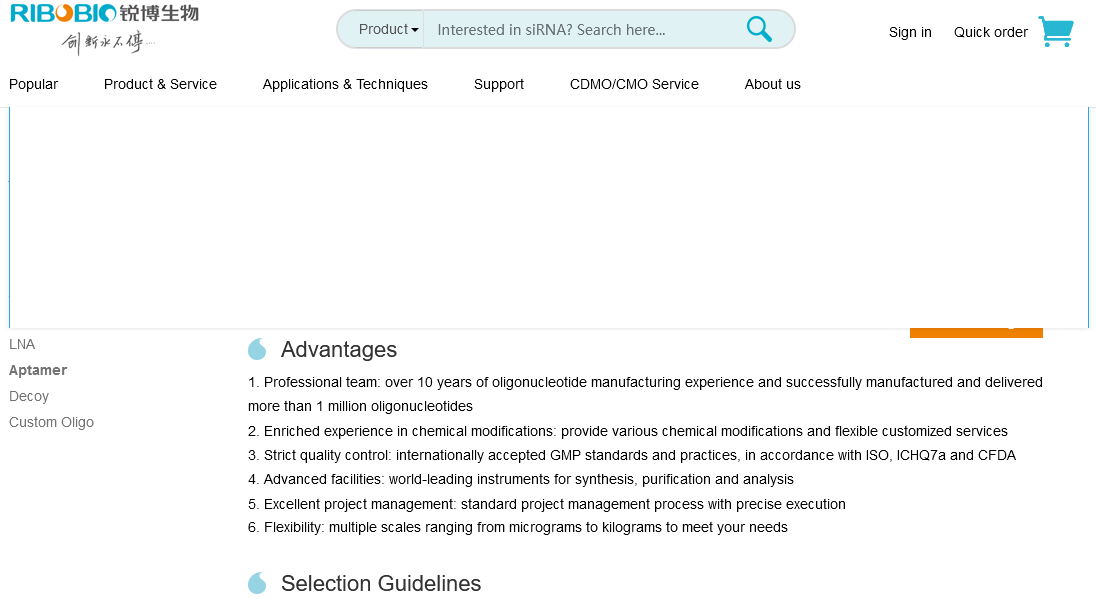
The results of the phase I clinical trial are the following:
A very simplified mode of action in heart cells can be seen in this video on their home page:
It sounds too good to be true.
Time will tell if BC007 is really worth being called the "German miracle" and the worldwide media hype.
2. Removal of the agonistic autoantibody from the bloodstream
Apheresis techniques for extracorporeal blood purification are used on a large scale for for a wide variety of indications. The best-known procedure is dialysis, in which the apheresis system acts as an artificial kidney. Immunoadsorption removes components of the immune system from the blood from the bloodstream and is an efficient therapy option for autoimmune diseases. A number of autoimmune diseases cannot be treated with drugs or are or only inadequately treatable with drugs. These include the autoimmune dilated cardiomyopathy. In this heart disease, agonistic autoantibodies against the β1-AR play a fatal role. The therapeutic immunoadsorption was used for the first time with great success in an autoimmune event directed against a GPCR (19). Removal of the antibodies resulted in a significant and, in most cases, long-term stable improvement in cardiac performance (20). The improvements in myocardial function and myocardial morphology were so extensive in some patients, that heart transplantation was not necessary. Interestingly, in the majority of cases, there is no new formation of autoantibodies.
Apheresis is the most cost intensive treatment with at least 2000 € per session. The number of sessions depends on the severity of the symptoms. Assuming that some filters cost around 7000 € and is used for 5 sessions, you'll end up spending 17.000 €. I've read a lot on a post-vax forum and it seems that it helps more with the neurological issues such as brain fog, not so much the cardiac ones although they are obviously connected to each other. Some patients felt even worse initially after the apheresis and a "reinfection" with the "virus" seemed to bring back all the symptoms, albeit with a lower severity. One patient even claimed that he might be cured after the 2nd session as all his symptoms have disappeared (haven’t heard from him afterwards). I also know someone in person who received one inuspheresis session that felt initially worse. But after a few days his symptoms slightly decreased, but came back with a lower severity after a reinfection with the so called "virus".
From my understanding apheresis only filters microclots, inuspheresis is more selective towards the agonistic autoantibodies.
However, my assessment remains the same: with all mixed the reviews and the high price I personally don't consider getting this treatment. Yes, there are different filters, but would you pay 7000 € for the filter alone without even knowing that the treatment will actually help you? I don't blindly trust the reviews in forums for the apharesis/inuspheresis. Therefore, I reckon that economic interests are more important than healing of the patient.
____________________________________________________
In my post about graphene derivates I mention another mechanism of damage of graphene oxide:
An article named "Endoperoxides Revealed as Origin of the Toxicity of Graphene Oxide" stated that EDTA does not influence the endoperoxides induced by GO, but an oligonucleotide linked with a fluorescein derivative significantly decreased the reactivity. Enter the following quote into Sci-Hub: “DOI: 10.1002/anie.201507070”
The problem with the oligonucleotide is that they didn't disclose the structure for a good reason. If someone can find this out, please post it in the comment section, so I can update this post.
Could BC007 also be beneficial for post-vax patients? A little background check revealed the following
BC-007 (aka ARC183) is a single-stranded DNA oligonucleotide aptamere originally developed as a thrombin inhibitor in the US and then re-purposed as a broad spectrum neutralizer of G-ProteinCoupled Receptor (GPCR) auto-antibodies in cardiomyopathy by a research team around Gerd Wallukat (then at the Max-Delbrück-Centrum for molecular medicine in Berlin/Germany), now working at the German biotech start-up Berlin Cures.[1], [2]
https://www.kinder-verstehen.de/wp-content/uploads/BC007_miracle_in_need_of_explanation_141221.pdf
Archemix Corp. and Nuvelo, Inc. announced that they have closed a Phase 1 clinical trial evaluating ARC183 as an anticoagulant for potential use in acute cardiovascular settings such as coronary artery bypass graft (CABG) surgery. Preliminary results from the trial show that administration of ARC183 resulted in a rapid onset of anticoagulation, demonstrated stable, dose-related anticoagulation activity and that the effects of the drug rapidly reversed after administration of the drug infusion ceased. However, the amount of drug needed to achieve the desired anticoagulation for use in CABG surgery resulted in a sub-optimal dosing profile. For that reason, the companies have decided not to pursue development of ARC183, and instead are actively pursuing an optimized second generation molecule.
I don't know which company will synthesize BC007 (ARC183) once the manufacturing authorization is granted, but a company that is capable to synthesize this aptamer at such a large scale might be this one:
I remain hopeful, but at the same time sceptic as a lot of desperate vax damaged people can't wait for the "cure". Maybe there is no cure and we are totally doomed. If BC007 turns out to be a failure, then you know what NOT to take.
The substacker Spartacus claims that a cure for the novel virus already existed a decade ago:

It's an interesting read. You can make your own opinion about DRACO on how legit it is. If DRACO is indeed the cure I'm sure it would have been removed from all search engines and encyclopedias.
I didn’t realize you were suffering from heart stuff too. It sounds like you and I have a lot in common. I just posted my contaminated “pure blood” And I’ll post again after I complete my second week of treatment here. Are you able to make it to Yelm to see Dr Ana? She’s the only doc I know of that’s fully treating contamination
Sending you lots of prayers 💓
I feel so sad that innocent souls have been damaged by the bastards in lab coats and their masters in Savile Row suits. Wishing you well in your quest for the truth and health. You are helping others in your endeavour, which is more than can be said of the pharmaceutical companies, the administrators who are supposed to protect us and the politicians who sit back and say nothing, or worse.